Free DD 2870 Form
Form Preview Example
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
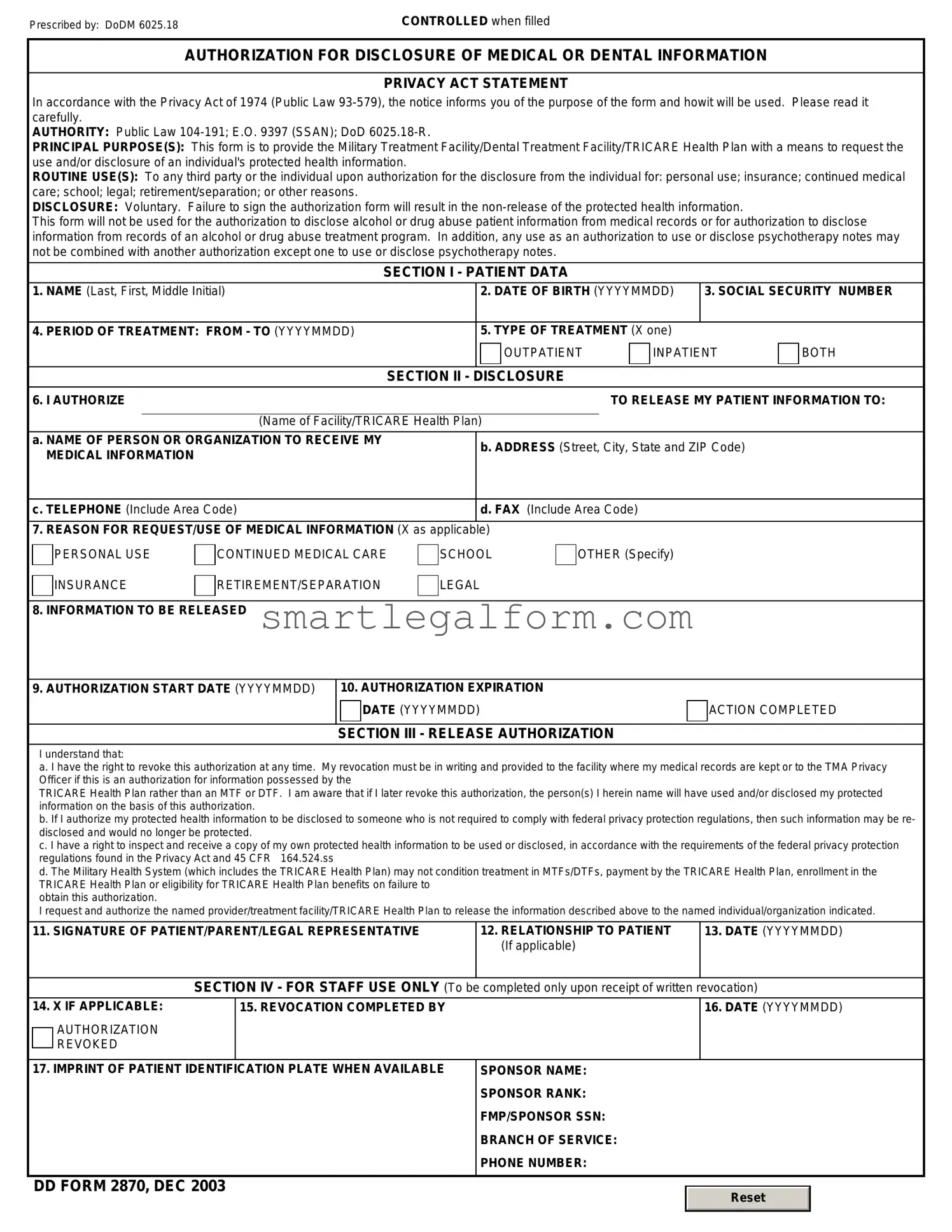
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Common mistakes
The DD 2870 form is essential for individuals seeking to authorize the release of their medical records or information. However, many people encounter challenges when filling out this form. One common mistake is not providing complete personal information. It is crucial to include your full name, address, and contact details accurately. Missing or incorrect information can lead to delays in processing your request.
Another frequent error involves misunderstanding the purpose of the form. Some individuals fill out the DD 2870 without realizing it is specifically for the release of medical records. This can result in requests being denied or misdirected. Understanding the form's intent helps ensure that the right information is requested.
People often neglect to specify the exact records they wish to obtain. The form allows for detailed descriptions, and failing to provide this information can lead to confusion. Without clarity, the records department may not know which documents to release, causing further delays.
Additionally, individuals sometimes overlook the signature requirement. The DD 2870 must be signed by the person authorizing the release of information. An unsigned form will be rejected, and the request will not be processed. This simple oversight can significantly prolong the time it takes to receive the needed records.
Another mistake is not providing the necessary identification. Many agencies require proof of identity to release medical records. Without this documentation, your request may be denied. It is essential to check the specific requirements of the organization handling the records.
People also frequently fail to read the instructions thoroughly. The DD 2870 comes with guidelines that explain how to fill it out correctly. Ignoring these instructions can lead to errors that could have been easily avoided. Taking the time to review the guidelines ensures that the form is completed accurately.
Finally, individuals may not follow up on their requests. After submitting the DD 2870, it is advisable to check in with the records department to confirm receipt and inquire about the processing timeline. This proactive approach can help address any issues that may arise and ensure that you receive the necessary information in a timely manner.
Dos and Don'ts
When filling out the DD 2870 form, it is important to follow certain guidelines to ensure accuracy and completeness. Here is a list of things to do and not to do:
- Do read the instructions carefully before starting.
- Do provide accurate personal information, including your full name and contact details.
- Do use black or blue ink when filling out the form.
- Do double-check all entries for spelling and numerical errors.
- Do sign and date the form where indicated.
- Don't leave any required fields blank; fill them out completely.
- Don't use abbreviations unless specified in the instructions.
- Don't submit the form without reviewing it for completeness.
- Don't forget to keep a copy of the completed form for your records.
- Don't rush through the process; take your time to ensure accuracy.
Other PDF Documents
Esa Letter for Anxiety - The documentation can ease living situations in no-pet housing environments.
In addition to its fundamental role, the FedEx Bill of Lading form can be conveniently accessed and downloaded online to streamline the shipping process. For those looking to utilize this form, it is available at https://documentonline.org/blank-fedex-bill-of-lading, ensuring that shippers have quick access to the necessary documentation.
Print Payroll Checks - Payroll Check forms can be produced in bulk for larger organizations.
Similar forms
The DD 2870 form is used for requesting access to military records and benefits. Here are nine other documents that are similar to the DD 2870 form, along with a brief explanation of how they relate:
- SF 180 - This form is used to request military records from the National Archives. Like the DD 2870, it facilitates access to personal military information.
- VA Form 21-4138 - This is a statement in support of a claim for veterans benefits. It serves to provide additional information, similar to how the DD 2870 supports requests for records.
- DD Form 214 - This document is issued upon separation from military service. It summarizes a service member's career and is often requested alongside the DD 2870 for benefits purposes.
- VA Form 21-526EZ - This form is for applying for veterans compensation and pension benefits. It requires information that may overlap with what’s provided in the DD 2870.
- SF 15 - This is a claim for 10-point veteran preference. It requires documentation similar to that requested in the DD 2870 to verify service.
- VA Form 21-530 - This form is used to apply for burial benefits. It can involve accessing military records, making it similar to the DD 2870.
- Form 22-5550 - This is a request for educational assistance for veterans. It often requires service documentation, like the DD 2870.
-
Texas Last Will and Testament - A legal document that specifies how assets should be distributed after death, ensuring the final wishes are honored. For more information, visit TopTemplates.info.
- DD Form 149 - This form is used to apply for a correction of military records. It shares the purpose of accessing and modifying military information.
- VA Form 21-8940 - This is an application for increased compensation based on unemployability. It may also require the submission of military service records, akin to the DD 2870.