Free Cna Shower Sheets Form
Form Preview Example
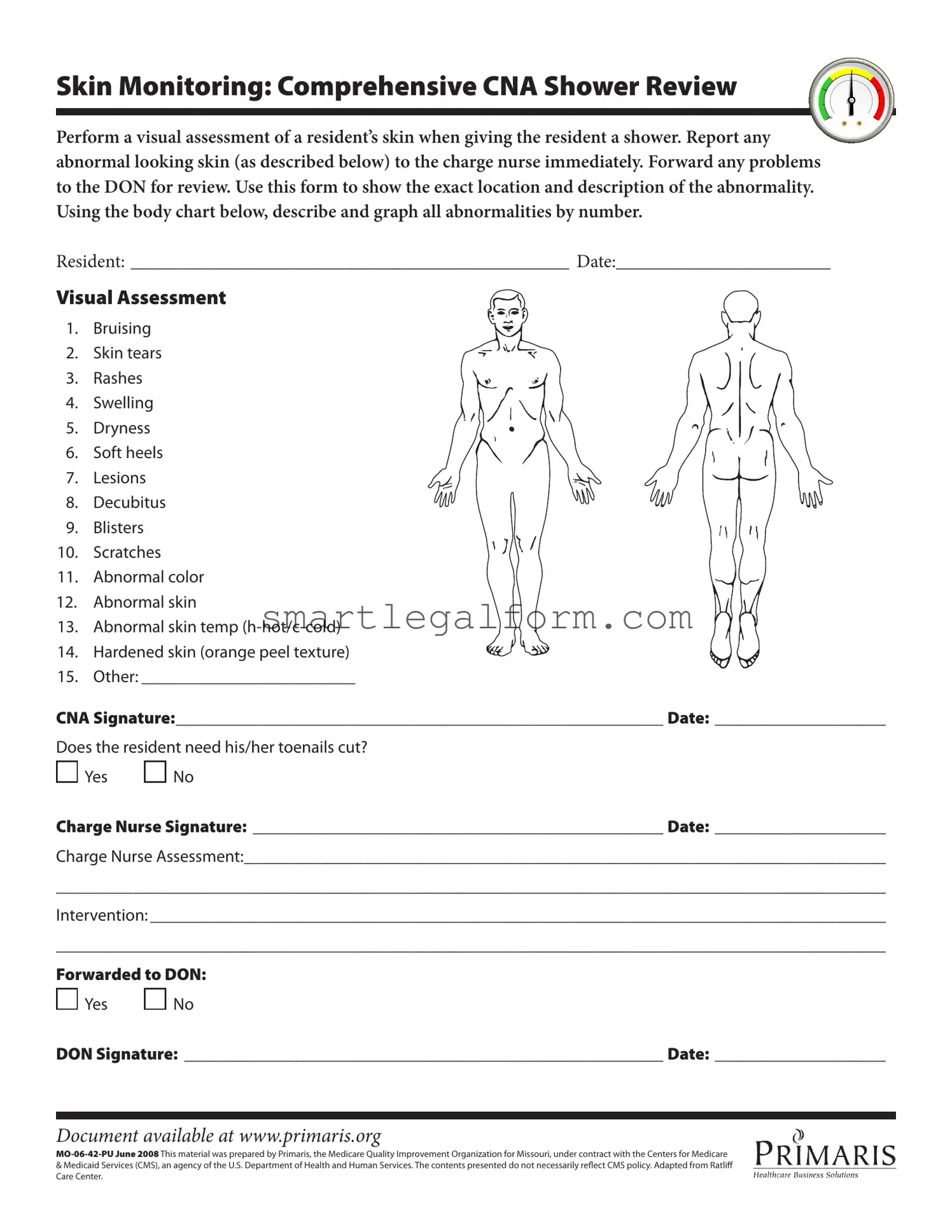
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Common mistakes
Completing the CNA Shower Sheets form accurately is essential for ensuring the health and safety of residents. However, many individuals make common mistakes that can lead to misunderstandings or inadequate care. One frequent error is failing to conduct a thorough visual assessment of the resident's skin. A comprehensive evaluation is crucial, as it allows for the identification of any abnormalities that may require immediate attention.
Another common mistake involves not reporting abnormal skin conditions promptly to the charge nurse. It is vital to communicate any findings immediately, as delays can result in further complications for the resident. Additionally, some CNAs may neglect to use the body chart provided to accurately describe and graph the location of abnormalities. This oversight can hinder the ability of healthcare professionals to assess the situation effectively.
Inconsistent terminology can also lead to confusion. For example, using vague descriptions such as "bad rash" instead of specifying the type of rash can result in miscommunication. Similarly, failing to document the exact date and time of the assessment can create gaps in the resident's medical history. Accurate documentation is essential for continuity of care.
Another error occurs when CNAs forget to sign the form. A signature is not merely a formality; it signifies accountability and professionalism. Furthermore, some individuals may overlook the section regarding toenail care. Not indicating whether the resident needs toenails cut can lead to neglect of this important aspect of personal hygiene.
In addition, CNAs sometimes fail to provide a detailed charge nurse assessment. This section is critical for outlining any interventions that may be necessary. If this information is lacking, it can impede the quality of care the resident receives. Lastly, not forwarding the form to the Director of Nursing (DON) when required can prevent essential follow-up actions from taking place.
Awareness of these common mistakes can help improve the accuracy and effectiveness of the CNA Shower Sheets form. By taking the time to review and complete the form diligently, CNAs can contribute significantly to the well-being of the residents they care for.
Dos and Don'ts
When filling out the CNA Shower Sheets form, it is essential to follow specific guidelines to ensure accuracy and clarity. Here are some dos and don'ts to keep in mind:
- Do perform a thorough visual assessment of the resident's skin during the shower.
- Do report any abnormalities to the charge nurse immediately.
- Do use the body chart to accurately describe and graph any abnormalities.
- Do ensure that all sections of the form are completed before submitting.
- Don't use vague language when describing skin issues; be specific.
- Don't forget to sign and date the form after completion.
- Don't leave any questions unanswered, especially regarding toenail care.
Other PDF Documents
Family Law Financial Affidavit Short Form Florida - This form helps prevent disputes over financial matters by laying everything out clearly.
The importance of the Employment Verification Form extends beyond just confirming employment history; it can also be accessed at documentonline.org/blank-employment-verification-form for those looking to familiarize themselves with the necessary requirements and procedures for completion, ultimately aiding in a smoother hiring process.
Baseball Evaluation Sheets - Trusted scoring criteria ensures that coaches remain aligned in their evaluation processes across teams.
Similar forms
The CNA Shower Sheets form serves a specific purpose in monitoring residents' skin health during showers. Several other documents share similar functions, focusing on health assessments and care documentation. Here are four documents that are similar to the CNA Shower Sheets form:
- Skin Assessment Form: This document is used to evaluate the overall condition of a resident's skin. Like the CNA Shower Sheets, it requires detailed observations and descriptions of any abnormalities, ensuring that caregivers can track changes over time.
- Incident Report Form: When a resident experiences a fall or injury, this form documents the incident. Similar to the CNA Shower Sheets, it emphasizes the need for immediate reporting and thorough documentation of observed issues to ensure proper follow-up and care.
- Hold Harmless Agreement: This agreement, commonly utilized in Florida, helps mitigate liability concerns during activities involving risks, ensuring that parties can engage in practices safely. For more information, refer to TopTemplates.info.
- Care Plan Review Document: This form outlines the individualized care plans for residents. It parallels the CNA Shower Sheets by incorporating specific observations related to skin health, allowing caregivers to adjust care strategies based on documented assessments.
- Daily Nursing Progress Notes: Nurses use this document to record daily observations and changes in a resident's condition. Like the CNA Shower Sheets, it highlights the importance of continuous monitoring and documentation of any health concerns to facilitate effective communication among the care team.